THE EXCHANGE | Newsletter November 2018
Medanta Launches Unique Therapeutic Approach with Medanta - AyurVAID:
Medanta - The Medicity in collaboration with AyurVAID Hospitals has launched Medanta-AyurVAID. Developed on a unique approach which optimizes a fusion of modern medicine and ancient disciplines of therapy, Medanta AyurVAID is a revolutionary concept. India's first NABH accredited Ayurveda hospital, AyurVAID is centered around precision Ayurveda that complements modern medicine.
Announcing the launch of Medanta-AyurVAID, Dr. Naresh Trehan, Chairman and Managing Director, Medanta said, ''Medanta's collaboration with AyurVAID Hospitals reinforces our practised belief in integrated medicine which draws from a variety of medical disciplines to craft unique, effective, customized therapeutic solutions. The synergistic approach ensures holistic treatment for effective root cause disease reversal and sustained wellbeing.”
In addition to the existing range of Ayurveda led services including consultations, medicines, out-patient therapies and therapeutic yoga, Medanta-AyurVAID offers in-patient medical care for patients suffering from serious non-communicable and chronic diseases including diabetes and other lifestyle disorders, arthritis and other musculoskeletal disorders, neuro-degenerative disorders, respiratory disorders, gynecological disorders, paediatric developmental disorders etc. Integration with other specialties and co-managed care reinforces efficacy and quality of treatment.


- Respiratory Disorders
- Paediatric Health
- Cancer Rehabilitation
- Skin & Hair Conditions
-
Women's Health
- Eye Disorders
- Pregnancy Care
- Reproductive Health
- Elder Care
- Ear Disorders
- Pre & Post-surgical Rehabilitation
- Nose Disorders
- Renal Disorders
- Lifestyle & Metabolic Disorders
- Gastrointestinal Disorders
- Mental Health & Deaddiction
- Musculoskeletal & Neurological Disorders
- Throat Disorders
In Good Hands
Leveraging the tactile abilities of visually impaired women in clinical setting, Dr. Frank Hoffmann, introduced the 'Discovering Hands' program in Germany in 2005. The program trains blind women in medical tactile examination. Using their highly developed tactile sense, medical tactile examiners (MTEs) can identify the minutest abnormalities in breasts at an early stage.
Tactilography has many scientifically proven successes: MTEs trained on specially developed, standardised and quality-assured concept of examination feel about 30 percent more tissue changes than doctors. This is a successful model followed in Germany, Austria and Columbia.
In India, the course has been conducted for the first time by the National Association for the Blind (NAB) which has expertise of training blind women in different vocations.
Prior to starting the course, numerous deliberations were held between different stakeholders, including scientists from Public Health Foundation of India (PHFI), Indian Cancer Society, National Association of Blind Delhi etc.
Dr. Kanchan Kaur, expert doctor on this panel, travelled to Germany and worked extensively on adapting the program to Indian settings. The nine-month course which has built-in aspects of medical training and patient orientation was conducted in India by trainers who were trained at the Germany 'Discovering Hands' facility. The first batch of five students was trained to use a specially designed computer software called Documentation and Orientation System

(DOKOS) to document patient details and findings, using medical terminology. After clearing their theory exams, they interned with Dr. Kanchan Kaur at the Medanta Breast Clinic. Patients examined by the MTEs gave a very positive feedback about their experience.

MTEs use innovative tactile orientation strips (based on Braille), developed by ‘Discovering Hands’ to perform the scanning tests. During the examination, five of such special adhesive strips are placed around a woman's breast that allow any abnormality to be detected by two dimensional coordinates. This allows the visually impaired MTEs to carry out breast examination independently. An examination typically lasts 20-30 minutes in which the MTE records patient history, conducts the examination and counsels on the importance of self-breast examination.
“In the Indian setting where 80% patients arive at a late stage due to widespread ignorance and misinformation, early detection is key to improved treatment outcomes. Over a period of time, as we train more MTEs, they could prove to be a useful adjunct to outreach and 'in-hospital' screening programs, also transforming their perceived disability into capability.”
Dr Kanchan Kaur,
Associate Director, Breast Services
Cancer Institute
https://www.medanta.org/dr-kanchan-kaur/
Neuro-intervention in Ischemic Stroke
Stroke is a leading cause of mortality and major disability in most countries. The lifetime risk of stroke after 55 years of age is 1 in 5 for women and 1 in 6 for men. More than four-fifth of all strokes occur in developing countries and an increasing trend of younger population getting affected is alarming.
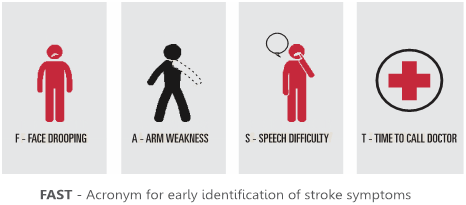
Typically in a stroke, depriving oxygen and blood supply to the brain results in immediate cell microstructure change and it stops functioning. In stroke management, thus, time is brain. Each passing minute following a stroke, millions of neurons are lost if obstructed clot is not dissolved or removed. Identification of early stroke symptoms like arm or leg weakness, face deviation and /or speech difficulty (FAST) is critical for timely intervention and complete recovery.
Endovascular mechanical thrombectomy (MT) within the window period is a crucial neurointervention for deficit free outcome. Recent multiple trials (DAWN, DEFUSE-3) have extended the intervention window from 6 to 24 hours in selected patients with penumbra (salvageable brain tissue), a welcoming move from ‘time’ to ‘tissue’ based treatment. Modern neurointervention and endovascular techniques have revolutionised stroke treatment. From simple stent retriever, we have evolved to other effective, early first pass reperfusion technique like our own master-hand DAFT (dual aspiration with push and fluff technique). The Medanta Institute of Neurosciences is one of the few Level 1 Centres of South-East Asia offering 24x7x365 tertiary referral stroke care.

Cath Lab, Medanta - The Medicity
Case Study
A 46-year-old male presented in the emergency complaining of acute onset of left sided limb weakness and facial deviation for 2 hours 40 minutes. He was a known case of hypertension, coronary artery disease (CAD), but non-diabetic. Prior to this incident, the patient was functionally independent. His physical examination revealed left lower limb power 1/5 and upper limb 2/5 with left UMN facial palsy. He was conscious but dull in verbal response with forced gaze deviation towards right. The National Institutes of Health Stroke Scale (NIHSS) was 12. The Emergency team at Medanta activated code ‘Brain Rescue’ in the triage and mobilized him for urgent stroke imaging. Non-contrast CT head showed very early ischemic changes in right frontal opercular area and no evidence of hemorrhage.
The Alberta Stroke Program Early CT Score (ASPECT) was 8.
His random blood sugar was 110 mg% and INR was 0.9.
The patient was administered weight based bolus dose of intravenous thrombolysis (recombinant tissue plasminogen activator, rtPA) in the imaging suite. The CT perfusion study showed large area of perfusion mismatched deficit in right MCA territory including the Rolandic motor strip, signifying penumbra. Angiography showed right MCA M1 occlusion.
The patient was immediately taken for mechanical reperfusion. Using solitaire stent retriever and ACE 68 aspiration catheter (DAFT technique), the clot was removed in a single pass with mTICI 3 reperfusion. Showing quick and early signs of recovery, the patient was able to lift his left sided limbs on the DSA table.
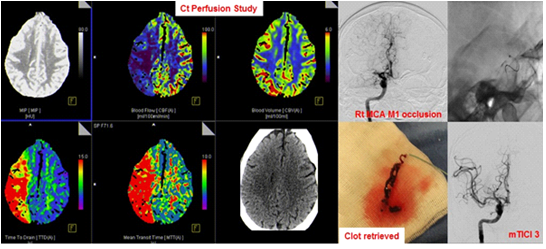
Acute stroke imaging (CT head and perfusion study) and neurointervention showing successful clot retrieval
Such immediate, comprehensive treatment was possible due to established, in-hospital comprehensive stroke care program.
In this particular patient, the Door to CT-Time (DTCT) was 12 minutes and Puncture to Reperfusion Time was 11 minutes, comparable to leading international stroke care centres. The patient was observed in stroke care unit and later worked-up for stroke etiology and risk factor stratification. His modified Rankin Scale (mRS) at discharge was one which dropped down to zero at 90 days follow-up.
Stroke is a medical and surgical emergency. It has major deleterious consequences for individuals, families, and society, if not treated timely. Stroke is preventable, treatable and more recently, curable in most patients.
Early identification of symptoms and treatment is critical to deficit-free outcome.
https://www.medanta.org/dr-gaurav-goel/